CPT Code 43235: Description, Cost, Scenarios, and Rules
| Quick Facts Table For CPT Code 43235 | |
|---|---|
| CPT Code | 43235 |
| Short Descriptor | EGD, diagnostic, with or without collection of specimen(s) by brushing or washing |
| Typical Place of Service | Both (facility and office/freestanding ASC) |
| Global Period | 0 days |
| PC/TC Split | No (PC/TC Indicator 0) |
| wRVU / Total RVU | ~3.69 wRVU / ~9.66 Non-Facility / ~3.31 Facility |
| Common Modifiers | 59, 22, 51, 76, 77, XS, XU |
| Medicare Payment (CY 2026) | $322.65 Non-Facility · $110.56 Facility |
Gastroenterology billing has its own language. Within that language, CPT code 43235 is one of the most frequently used terms. It appears on thousands of claims every week across hospitals, ambulatory surgical centers, and outpatient GI practices. And yet, it is also one of the most commonly miscoded codes in the specialty.
The reason is not complexity. It is precision. CPT 43235 has a narrow, specific meaning. When used correctly, it processes cleanly. When used incorrectly or when a more comprehensive code was warranted, it generates denials, audit flags, and lost reimbursement. Practices that invest in accurate gastroenterology billing services see a direct impact on clean claim rates for codes like 43235.
This guide walks through everything a billing professional, coder, or GI practice manager needs to know: what the code means, what it costs, how it behaves in real billing scenarios, and what rules govern its use.
What is CPT Code 43235?
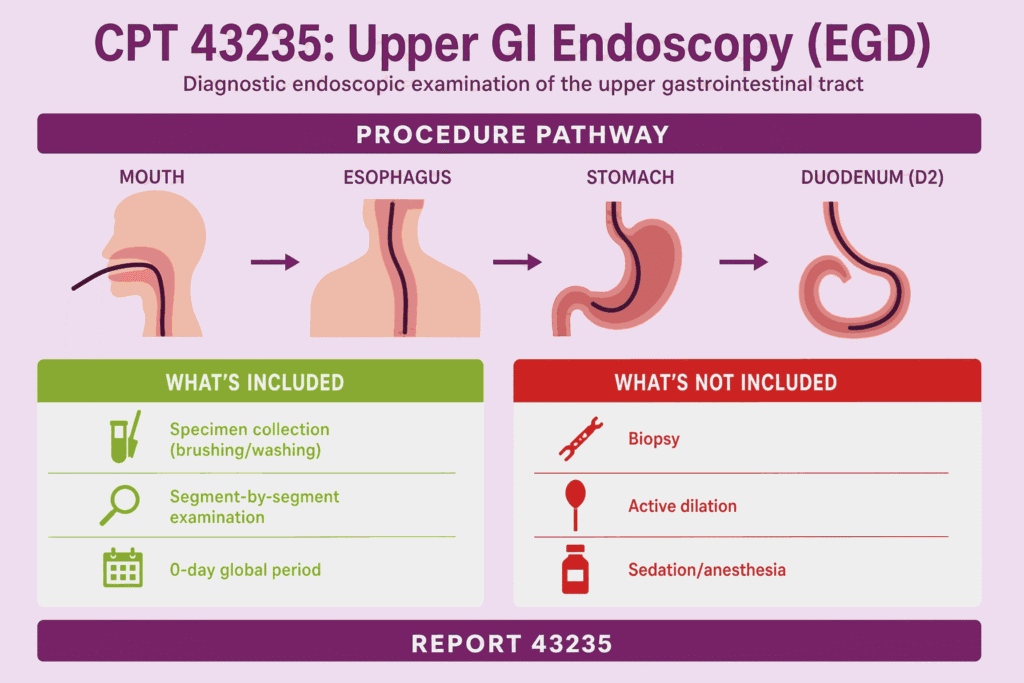
CPT code 43235 is used for a diagnostic upper gastrointestinal endoscopy procedure. This procedure allows the physician to examine the upper digestive tract using a flexible scope. This procedure is commonly referred to as an EGD, or esophagogastroduodenoscopy.
The full descriptor reads: esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed.
That final phrase matters. The code permits specimen collection by brushing or washing as an included component. It does not permit a biopsy. If a tissue sample is taken and sent to pathology, you are no longer in 43235 territory. The procedure has crossed into a different code family.
CPT 43235 remains a 0-day global period service. This means there is no post-procedure follow-up bundled into the payment. An E/M service on a separate date following the EGD can be billed independently, as long as documentation supports a distinct, separately identifiable visit.
Procedure Overview: Upper GI Endoscopy with Dilation
The procedure itself begins with the patient receiving conscious sedation or monitored anesthesia care, administered by a separate provider. The gastroenterologist introduces the flexible endoscope transorally, meaning through the mouth. The scope travels down the esophagus, into the stomach, and advances into the proximal duodenum, specifically to the second portion known as D2.
The procedure involves examining the upper GI tract up to the duodenum, as well as the collection of specimen(s) through brushing or washing, if performed.
Throughout the examination, the physician documents findings segment by segment. The esophageal mucosa, the gastroesophageal junction, the gastric cardia, fundus, body, and antrum, and finally the duodenal bulb and second portion are all observed and recorded. When the title of this code references “dilation,” it refers to the anatomical scope of the instrument’s passage, not an active dilation procedure performed on a stricture. Active dilation is coded separately.
Anatomical Scope: Esophagus, Stomach, and Duodenum
The three-organ reach of CPT 43235 is what separates it from shorter upper endoscopy procedures. The esophagus is examined for signs of esophagitis, Barrett’s changes, varices, or stricture. The stomach is inspected for gastritis, ulceration, polyps, and H. pylori-associated changes. The duodenum is evaluated for duodenitis, ulcers, and villous abnormalities.
Documentation must reflect all three segments. A note that says “EGD performed, unremarkable” is not sufficient. Payers and Medicare Administrative Contractors increasingly require segment-by-segment documentation to support medical necessity. This is not a suggestion. It is a pattern that drives denials when ignored.
Sedation, if administered by a CRNA or anesthesiologist, is billed separately using the appropriate anesthesia codes. Moderate sedation during the EGD procedure must be billed separately using appropriate sedation codes. This is a billing consideration that trips up newer practices: the sedation is not included in the 43235 reimbursement.
Difference Between Diagnostic and Therapeutic EGD
This distinction is the single most important concept for anyone coding upper GI endoscopy. CPT 43235 is strictly for diagnostic procedures. If the physician performs any additional intervention during the procedure, a different CPT code should be used.
Diagnostic means the scope was used for observation and evaluation. The physician looked. They may have performed brushings or washings. Nothing was removed, injected, cauterized, dilated mechanically, or biopsied.
Therapeutic means the physician did something beyond observation. A biopsy moves the code to 43239. Hemostasis by injection or thermal method moves it to 43255 or 43227, depending on the technique. Active dilation using a balloon or bougie has its own code family. Polypectomy by hot biopsy forceps is coded at 43250. Snare polypectomy at 43251.
The core rule is this: surgical endoscopy includes diagnostic endoscopy. If a more extensive upper GI endoscopic service is performed, report only the single most comprehensive code; never stack 43235 with another EGD family code.
If the physician performed a biopsy during the same session that otherwise would have been a diagnostic EGD, do not report 43235 plus 43239. Report 43239 only. The diagnostic component is included in the therapeutic code. Understanding how these codes interact is foundational to accurate gastroenterology billing and preventing unnecessary denials across upper GI claims.
Average Cost of CPT 43235 Without Insurance
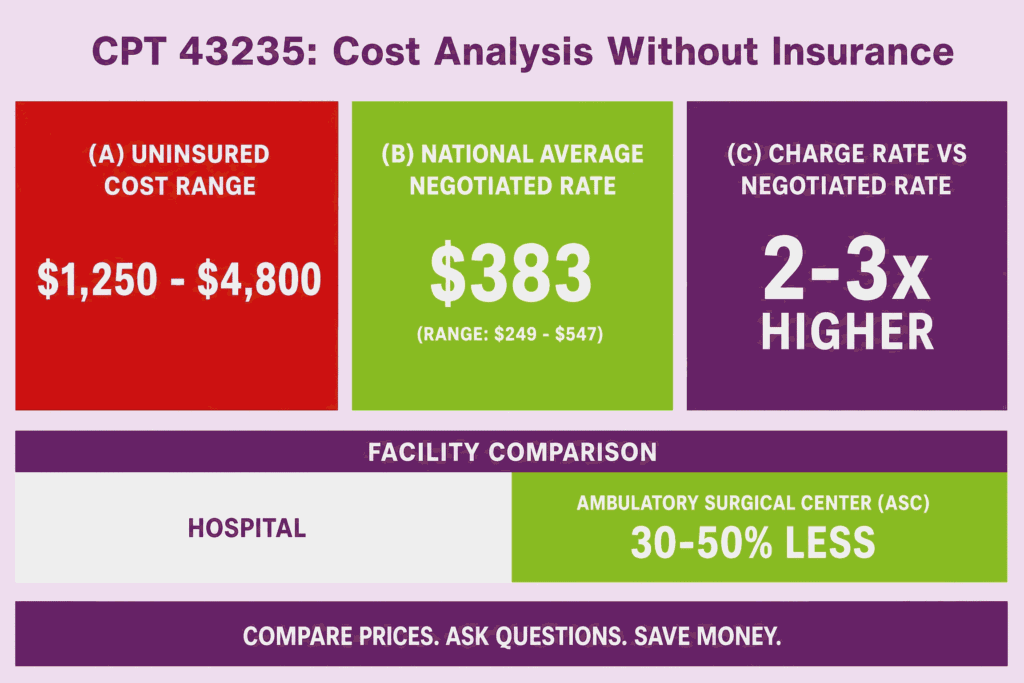
Without insurance, this procedure can cost between $1,250 and $4,800. These costs typically cover the fee for the physician performing the endoscopy, the anesthesiologist, and the facility.
Outpatient surgery centers typically charge 30 to 50 percent less than hospital outpatient departments. A patient presenting at a hospital-based endoscopy suite in a major metropolitan area will face a substantially different bill than a patient seen at a freestanding ambulatory surgical center in a mid-sized city.
The average negotiated rate for an upper endoscopy under CPT 43235 is $383 nationally, with rates typically ranging from $249 to $547 depending on state and provider. Without insurance, the patient may pay the provider’s full charge rate, which can be two to three times higher than the negotiated rate.
This gap between charge rate and negotiated rate is an important context for billing teams. The figure on the claim form is not what anyone actually collects. Payer contracts, locality adjustments, and facility agreements all compress that number significantly.
Medicare Reimbursement Rate for CPT 43235
For 2026, the estimated national average Medicare payment for CPT 43235 is $322.65 in a non-facility (office) setting and $110.56 in a facility (hospital or outpatient) setting. The code carries 9.66 total RVUs in the non-facility setting and 3.31 total RVUs in the facility setting.
The gap between non-facility and facility rates reflects a foundational Medicare payment principle. When a procedure is performed in a physician’s private office, the physician absorbs the overhead: equipment, supplies, staff, and space. Medicare compensates for that with a higher physician fee. When the procedure is performed at a hospital or ASC, the facility bills its own fee separately, so the physician component drops sharply.
This reflects a 16.80 percent change from the prior year. For GI practices tracking year-over-year revenue, this is a meaningful shift. Budget projections built on prior-year rates for 43235 in non-facility settings need to be updated.
Medicare pays 80 percent of the allowed amount. The remaining 20 percent is the patient’s coinsurance responsibility, absent a supplemental policy. When enrolling as a participating provider, you are required to bill on an assignment basis and accept the Medicare allowable fee as payment in full. Medicare will pay 80 percent of the allowable amount, and the patient will pay a 20 percent coinsurance.
Medicaid and Commercial Payer Payment Ranges
Medicaid rates for CPT 43235 vary significantly by state. Most state Medicaid programs pay below Medicare rates. Some states pay as low as 60 to 70 percent of the Medicare fee schedule. Practices that treat a high volume of Medicaid patients need to account for this in their revenue models, particularly when calculating contribution margin per procedure.
Commercial payers, including major carriers like UnitedHealthcare, Aetna, Cigna, and BCBS plans, negotiate rates based on contract terms with individual practices and health systems. In most markets, commercial rates sit above Medicare for CPT 43235, though the spread varies. A large GI group with leverage in a concentrated market may negotiate 130 to 160 percent of Medicare. A solo practitioner in a competitive urban market may negotiate closer to Medicare parity.
With insurance, out-of-pocket costs after meeting a deductible can range from $500 to $2,000, depending on the plan, with coinsurance typically falling between 10 and 40 percent.
Facility vs. Physician Fee: How Costs Are Split
When CPT 43235 is performed at an outpatient hospital or ASC, the total cost is split across two separate claims. The physician bills the professional component using Place of Service 22 (outpatient hospital) or 24 (ASC), triggering the reduced facility rate. The hospital or ASC bills its own facility fee using the applicable APC (Ambulatory Payment Classification) under the OPPS system.
These are separate claims, submitted by separate entities, reimbursed under separate fee schedules. Patients sometimes receive two or more explanations of benefits documents for the same procedure and find the dual billing confusing. Billing staff frequently need to explain why two claims exist for what the patient experienced as a single visit.
The facility fee for an ASC is typically lower than what the hospital outpatient department receives. CMS payment policy has historically favored ASC settings for cost reduction, making them an attractive option for payers and patients seeking lower out-of-pocket costs.
Patient Out-of-Pocket Responsibility
A patient’s actual out-of-pocket cost depends on four variables: whether the deductible has been met, the coinsurance percentage under their plan, whether the provider is in-network, and whether any secondary coverage applies.
In 2026, many insurers will require prior authorization for endoscopy. Without it, coverage may be denied. This is a newer development. Historically, diagnostic EGDs in patients with established symptoms moved through without pre-auth. That has changed. Practices that skip prior authorization workflows for 43235 are seeing claim denials that could have been prevented at the front end of the revenue cycle.
For self-pay patients, negotiated cash prices at freestanding ASCs can reduce the total cost substantially. Some private clinics offer all-inclusive packages starting at $1,200 for a diagnostic EGD. Transparency in Coverage data, available through most insurer portals, now allows patients to look up negotiated rates before scheduling.
CPT Code 43235 Scenarios
Scenario 1: Billing 43235 for Esophageal Stricture Dilation
A 58-year-old patient presents with progressive dysphagia for four months. The referring physician suspects a benign esophageal stricture based on barium swallow results. The gastroenterologist performs an EGD and identifies a stricture at 30 cm from the incisors. The physician performs a diagnostic examination, documents the stricture, and ends the procedure.
In this session, no dilation is performed. The scope passes the structure for observation. Code 43235 is appropriate. The documentation must capture the anatomical location of the stricture, its estimated length and severity, and the endoscopist’s clinical impression.
Now change the scenario. The same patient presents. The gastroenterologist identifies the stricture and proceeds to dilate it using a through-the-scope balloon. This is no longer a diagnostic procedure. The appropriate code shifts to 43220 (esophageal dilation, without guidewire) or 43249, depending on the technique used. Billing 43235 in this second scenario would be undercoding at best and a documentation mismatch at worst.
The lesson: review the operative report before assigning 43235. If any intervention occurred beyond visualization and brushings or washings, a higher-level code is required.
Scenario 2: Using 43235 With a Secondary Diagnosis Code
A patient is referred for evaluation of persistent nausea, early satiety, and unintentional weight loss over three months. The EGD is performed. Findings show mild antral gastritis without erosion. No biopsy is taken. No other intervention is performed.
CPT 43235 is the correct procedure code. The primary diagnosis code is the symptom driving the procedure. The secondary code supports the finding: K29.70 (gastritis, unspecified, without bleeding) or the more specific K29.60 (other gastritis without bleeding), depending on the endoscopist’s documented impression.
ICD-10-CM codes must support medical necessity and provide coverage for CPT code 43235. The symptom-based codes (R11.0 for nausea, R11.10 for vomiting, K21.0 for GERD with esophagitis) are among the most commonly linked diagnosis codes for this procedure. The diagnosis code is not cosmetic. It is the mechanism through which the payer evaluates whether the procedure was appropriate.
If the diagnosis code does not appear on the payer’s covered diagnosis list for 43235, the claim will be denied on medical necessity grounds regardless of how well the operative note is written.
Scenario 3: 43235 in an Outpatient Hospital Setting
A patient is scheduled for a diagnostic EGD at a hospital-based outpatient endoscopy unit. The procedure is performed and coded as 43235. The physician bills the professional service with Place of Service 22. The hospital bills the facility fee under the OPPS.
The physician reimbursement in this setting is the facility rate: $110.56 at the national average for 2026. This is the number the practice should build into per-procedure contribution analysis. The practice is not collecting $322.65 for this procedure. It is collecting $110.56 for the physician component, while the hospital bills separately for the facility portion.
In high-volume practices where a significant share of procedures occur in hospital-based settings, this rate difference has a meaningful revenue impact. The same procedure performed in a physician-owned ASC triggers a higher physician rate because the physician entity absorbs the overhead.
Documentation requirements in the outpatient hospital setting are the same as in any other setting. The operative report, pre-procedure note, and indication documentation must all be present in the medical record.
Scenario 4: When 43235 Is Bundled With Another Procedure
A gastroenterologist performs an EGD on a patient with hematemesis. During the procedure, they identify a bleeding gastric ulcer and inject epinephrine for hemostasis. The physician bills 43235 plus 43255 (EGD with control of bleeding by any method).
This is a bundling error. NCCI edits prevent stacking diagnostic and therapeutic codes in the same session. CPT 43255 includes the diagnostic component. Billing 43235 alongside it violates the principle that surgical endoscopy includes diagnostic endoscopy. The correct approach is to bill 43255 only.
A similar pattern applies to stent placement. CPT 43266, EGD with endoscopic stent placement, includes pre-dilation, post-dilation, and guidewire passage. These components are bundled and should not be billed separately. Unbundling 43266 with dilation codes remains a leading denial trigger. The same logic applies to 43235: if a more comprehensive therapeutic code was performed, that code stands alone.
Scenario 5: Modifier Use When 43235 Is Performed With 43239 or 43270
This is one of the more nuanced situations in upper GI coding. A patient undergoes an EGD during which the physician takes biopsies from the stomach and also evaluates the esophagus diagnostically.
The biopsy code, 43239, is the comprehensive code here. CPT 43239, EGD with biopsy, single or multiple, remains the highest-volume upper GI CPT code. Documentation must specify biopsy location, specimen count, and clinical reason. Billing 43235 alongside 43239 on the same claim, even with a modifier, is not appropriate. The biopsy code subsumes the diagnostic component.
Now consider 43270, which covers EGD with ablation of tumor, polyp, or lesion. If a physician performs ablation and nothing else, 43270 stands alone. The diagnostic examination is included. Modifier 59 or X modifiers should not be appended to unbundle 43235 from other upper GI endoscopy codes in the same session.
The use of modifier 59 for same-session, same-anatomic-region upper GI endoscopy codes is inappropriate regardless of how the claim is worded. Modifier 59 signals a distinct procedural service. When both codes are performed through the same transoral access, on the same anatomical structures, during the same session, the distinction does not exist.
CPT Code 43235 Billing Rules
CCI Edits and Bundling Restrictions for 43235
The Correct Coding Initiative edits govern which code combinations Medicare will pay for in the same session. For CPT 43235, the foundational rule is straightforward: it cannot be reported alongside another upper GI endoscopy code in the same session.
CMS updates bundling rules quarterly, making it essential for billing departments to stay current with changes. Updates can include new edit pairs, changes to existing pairs, or removal of obsolete pairs.
CPT 43889, endoscopic sleeve gastroplasty, was introduced in 2026. Do not report 43235 with 43889, as payers will deny both as bundled. This reflects the AMA’s effort to prevent double-billing when diagnostic EGD is performed as part of bariatric endoscopy.
The CCI table assigns each edit an indicator. Indicator 0 means codes are mutually exclusive and cannot be unbundled under any circumstance. Indicator 1 represents circumstances in which the edit can be unbundled. Some reasons for unbundling may be a different session or a different site. For upper GI endoscopy code pairs where both codes address the same organ system in the same transoral session, the modifier indicator is typically 0, meaning no modifier can override the bundle.
Documentation Requirements for Medical Necessity
Medical necessity documentation for CPT 43235 rests on three elements: the clinical indication, the procedure findings, and the plan following the procedure.
The indication must be specific. “Abdominal pain” without further context does not carry the same weight as “epigastric pain with nocturnal awakening, unresponsive to empiric PPI therapy for six weeks, with alarm symptoms of early satiety.” The more specific the clinical indication, the more defensible the claim is during audit review.
In 2026, vague notes such as ‘biopsy taken’ no longer satisfy medical necessity review and trigger audits. While this language refers to biopsy documentation in 43239, the same audit posture applies to 43235. Notes that state “EGD performed, scope advanced to duodenum, findings unremarkable, plan discussed” are insufficient. Findings must be segment-by-segment. Normals must be documented as normals.
The plan section of the note must follow from the findings. If the EGD was unremarkable and the indication was GERD symptom management, the note should document the clinical decision made based on the negative findings. Payers increasingly look at the clinical logic of the entire visit, not just the procedure code.
Modifier 59 and Unbundling Guidelines
Modifier 59 signals to the payer that a procedure or service was distinct and independent from another service billed on the same date. Perhaps the most widely used NCCI-related modifier, modifier 59, indicates that procedures or services that are not normally reported together were distinct or independent from each other. Because of potential overuse, CMS introduced X modifiers to provide more specificity.
The four X modifiers provide more granular documentation of why the distinctness exists: XE for separate encounter, XS for separate structure, XP for separate practitioner, and XU for unusual non-overlapping service.
When modifiers 59, XE, XP, XS, or XU are appended to a code, and there is an NCCI modifier indicator of 1, the payer will consider both reimbursement services.
For CPT 43235 specifically: modifier 26 or TC is not appropriate, as 43235 is a surgical endoscopy code, not a service with professional or technical splits like imaging. Modifier 51 is unnecessary for most payers and is not a workaround for endoscopy family bundling. It does not convert 43235 into a separately payable add-on. Modifiers 76 and 77 are rarely appropriate for 43235, as repeating the same endoscopic service in the same anatomic region during the same session is generally one unit only.
Payer-Specific Prior Authorization Requirements
Prior authorization requirements for CPT 43235 vary by payer and plan type. There is no universal standard. Medicare fee-for-service does not require prior authorization for diagnostic EGD. Medicare Advantage plans, on the other hand, may require it.
Commercial payers have been expanding prior authorization requirements for endoscopy procedures since 2022. The rationale is utilization management: payers want to confirm that the procedure is being ordered for a covered indication before the service is rendered.
In 2026, many insurers will require prior authorization for endoscopy. Without it, coverage may be denied. The denial in a prior authorization scenario is not clinical. It is an administrative denial. The procedure may have been entirely appropriate medically. The claim fails because a step in the workflow was skipped before the patient arrived.
Best practice is to verify prior authorization requirements at the time of scheduling. Build the prior auth check into the intake workflow. If a patient’s plan requires it and the EGD is elective, obtain authorization before the appointment. If the procedure is urgent, document the urgency clearly and follow the payer’s post-service authorization process.
Common Denial Reasons and How to Avoid Them
CPT 43235 denials cluster around five patterns.
Incorrect code selection. The physician performed a biopsy, but the coder defaulted to 43235 because the template used it as the starting point. The fix is mandatory operative report review before code assignment. Templates should not pre-populate procedure codes.
Medical necessity mismatch. The diagnosis code on the claim does not appear on the payer’s covered diagnosis list for 43235. The fix is to cross-reference the covered diagnoses in the applicable LCD before submitting. CMS publishes these under Article A57414 for upper GI endoscopy procedures.
Missing prior authorization. The payer required pre-auth, and the practice did not obtain it. The fix is a payer-specific prior auth matrix maintained by the billing team and reviewed at the time of scheduling.
Bundling error. The claim includes 43235 alongside a therapeutic EGD code performed in the same session. The modifier to bypass a CCI edit needs to be applied to the secondary code. And it is essential to have a valid justification for bypassing the edit. For same-session upper GI endoscopy bundles, a valid justification typically does not exist. The correct response is to remove 43235 from the claim.
Insufficient documentation. The operative note does not support the level of complexity implied by the clinical indication, nor does it document segment-by-segment findings. The fix is provider education. Notes must be complete before the claim is submitted.
Practices that build these checkpoints into their revenue cycle process see cleaner claim rates, fewer denials, and faster reimbursement. Those who rely on habit and default templates see the opposite. For a broader view of how these rules apply across upper GI procedures, refer to the complete guide on gastroenterology CPT codes.
Schedule your free MIPS demo.
Drop your work email and a certified MIPS consultant will reach out to schedule a personalized demo — no obligation.