MIPS Cost Category: Measures, Attribution, and Risk

The MIPS Cost category is the CMS-calculated, claims-based performance category that measures resource use under the Merit-Based Incentive Payment System (MIPS). The Cost category accounts for 30 percent of the 2026 MIPS final score across 35 measures: the Total Per Capita Cost (TPCC), the Medicare Spending Per Beneficiary (MSPB) Clinician measure, and 32 episode-based measures. Clinicians submit no Cost data; CMS calculates each score directly from Medicare Part B claims using attribution rules and risk adjustment.
What Is the MIPS Cost Category?
The MIPS Cost category is one of four MIPS performance categories under the Quality Payment Program (QPP), alongside Quality, Promoting Interoperability, and Improvement Activities. The Cost category is weighted at 30 percentof the 2026 MIPS final score and covers 35 cost measures in total. Unlike the other three categories, the Cost category is entirely CMS-calculated from Medicare Part B claims data. Clinicians do not submit Cost data through a registry, EHR, or attestation portal.
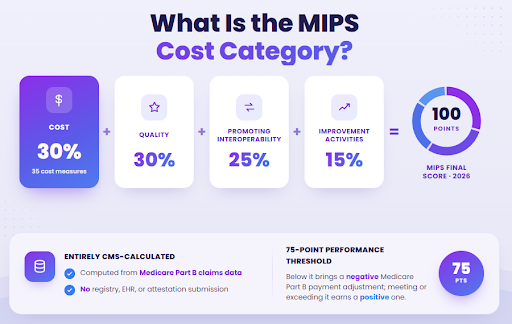
The four MIPS performance categories together form a 100-point MIPS Final Score. The 2026 weight distribution is: Cost at 30%, Quality at 30%, Promoting Interoperability at 25%, and Improvement Activities at 15%. The MIPS performance threshold for 2026 is 75 points. Clinicians scoring below the threshold face a negative payment adjustment; those above earn a positive adjustment to their Medicare Part B payments.
How Does Cost Contribute to the MIPS Final Score?
The Cost category contributes up to 30 points to the 100-point MIPS Final Score. CMS calculates a Cost category percent score by averaging the measure-level scores for each cost measure attributed to the clinician. That percent score is then multiplied by the 30% weight to produce the category’s point contribution to the MIPS Final Score. A clinician who scores 90% on Cost contributes 27 of the 30 available Cost points.
The remaining 70 points come from Quality (30%), Promoting Interoperability (25%), and Improvement Activities (15%). Each category is scored separately, and the four category scores are combined to produce the MIPS Final Score. Clinicians use their annual MIPS feedback report to review Cost performance before the applicable payment adjustment year.
Do Clinicians Submit MIPS Cost Data?
No, CMS calculates Cost performance directly from Medicare Part B claims. Clinicians do not submit any Cost data through a registry, EHR vendor, or the QPP portal. The no-submission rule applies only to Cost; the other three MIPS categories (Quality, Promoting Interoperability, and Improvement Activities) require active data submission by the clinician or the reporting group.
What MIPS Cost Measures Does CMS Use?
The 2026 MIPS Cost measure inventory contains 35 measures across three classes: 1 Total Per Capita Cost (TPCC) measure, 1 Medicare Spending Per Beneficiary (MSPB) Clinician measure, and 32 episode-based cost measures. CMS attributes each measure to a clinician based on the type of care delivered and the applicable attribution rules.
Clinicians may be attributed one, several, or all three measure classes depending on practice type and patient population. The three measure classes differ by trigger type, patient population, and attribution window:
| Measure Class | Count (2026) | Attribution Trigger | Care Focus |
|---|---|---|---|
| Total Per Capita Cost (TPCC) | 1 | Primary-care E/M visits (plurality) | Primary care, annual |
| Medicare Spending Per Beneficiary (MSPB) Clinician | 1 | Inpatient admission (admitting clinician) | Inpatient, episode window |
| Episode-based cost measures | 32 | Procedure or condition trigger code | Condition/procedure-specific |
| Total | 35 |
Each measure class uses a distinct attribution mechanism, and a single patient can generate attribution across multiple measure classes and TIN-NPIs in the same performance year.
What Is the Total Per Capita Cost (TPCC) Measure?
The Total Per Capita Cost (TPCC) measure is the primary-care-attributed cost measure that calculates the average annual Medicare Parts A and B costs across all patients attributed to a clinician through primary-care visits. TPCC attribution is based on the plurality of primary-care evaluation and management (E/M) visits. The clinician who bills the highest share of a patient’s primary-care E/M visits over the performance year receives TPCC attribution for that patient.
TPCC measures the total cost of care across all services, not only services that the attributed clinician delivers personally. That design reflects TPCC’s role as a resource-use measure: the attributed primary-care clinician is accountable for the full cost associated with coordinating care for attributed patients.
How Did TPCC Change for 2026?
CMS modified the TPCC measure for 2026 in the November 5, 2025, Physician Fee Schedule Final Rule. Candidate events initiated by Advanced Care Practitioner (ACP) TIN-NPIs are excluded when all non-ACP TIN-NPIs in the group are specialty-excluded. In practice, mixed physician-ACP groups where the physicians fall outside primary-care specialties are less likely to accumulate TPCC attribution under the 2026 rule.
Groups with mixed physician-ACP staffing should audit their TIN-NPI composition to determine whether the 2026 TPCC modification changes their attribution exposure before the performance year closes.
What Is the Medicare Spending Per Beneficiary (MSPB) Clinician Measure?
The Medicare Spending Per Beneficiary (MSPB) Clinician measure attributes inpatient-care spending to the clinician who serves as the admitting physician for a Medicare hospitalization. The MSPB Clinician episode window spans 3 days before the inpatient admission through 30 days after discharge. All Medicare Parts A and B claims within that window are included in the episode cost calculation.
MSPB Clinician is distinct from TPCC in both trigger and scope. TPCC is a longitudinal measure across a full performance year of primary-care visits. MSPB Clinician is an episode measure triggered by a single inpatient admission. A hospitalist or attending physician who regularly admits Medicare patients is likely to accumulate MSPB Clinician attribution; a primary-care-only outpatient practice typically does not.
What Are Episode-Based Cost Measures?
Episode-based cost measures attribute the total cost of a defined clinical episode to the clinician who billed the trigger code that initiated the episode. The 32 episode-based cost measures active for 2026 include Hip Replacement, Acute Myocardial Infarction (AMI), COPD Exacerbation, Knee Replacement, and Revascularization, among others. Each measure has a specific trigger code, an attribution rule, and a defined episode cost window.
Episode-based measures fall into two types:
- Procedure-triggered episodes: The trigger is a specific procedure code, such as a total hip arthroplasty CPT code for the Hip Replacement measure.
- Condition-triggered episodes: The trigger is a condition-related claim code, such as a COPD-related hospitalization code for the COPD Exacerbation measure.
The episode cost window includes all Medicare Parts A and B spending from the trigger date through the end of the defined episode period, regardless of which clinician delivered those services.
How Many MIPS Cost Measures Exist for 2026?
The 2026 MIPS Cost measure inventory contains 35 total measures: 1 TPCC measure, 1 MSPB Clinician measure, and 32 episode-based measures. CMS finalized one additional claims-based measure for 2026, but that measure carries informational-only status and does not contribute to the Cost category score.
The count of scoring-eligible measures is 35, unchanged from 2025 per the November 5, 2025, Physician Fee Schedule Final Rule.
Can a New MIPS Cost Measure Lower a Clinician’s 2026 Final Score?
No. Beginning with performance year 2026, any new cost measure CMS finalizes enters a 2-year informational-only feedback period before contributing to the Cost category score or MIPS Final Score. Clinicians receive performance feedback on a new measure during the two informational years, but the measure carries zero scoring weight during that period. Standard scoring for a new measure begins in year 3 of the measure’s existence under MIPS.
How Does CMS Attribute a MIPS Cost Measure to a Clinician?
Attribution is the process CMS uses to assign a patient (for TPCC) or a clinical episode (for episode-based measures) to a specific clinician at the TIN-NPI level. CMS assigns attribution based on candidate-event rules that differ across the three measure classes. The unit of attribution is always the TIN-NPI combination: the clinician’s individual National Provider Identifier (NPI) paired with the Tax Identification Number (TIN) of the practice under which the service was billed.
The attribution process runs automatically from Medicare Part B claims data after the performance year ends. Clinicians do not submit attribution requests. Attribution results are published in the annual MIPS Cost feedback report from CMS and are available through the QPP portal.
What Is a Candidate Event in MIPS Cost Attribution?
A candidate event is a billed service that triggers the attribution logic for a given MIPS Cost measure. For TPCC, the candidate event is a primary-care evaluation and management (E/M) visit billed by the clinician during the performance year. For episode-based measures, the candidate event is the procedure or condition trigger code that initiates the episode cost window.
Specialty exclusion rules apply to candidate events. If a clinician’s specialty code appears on CMS’s specialty-exclusion list for a given measure, candidate events billed by that clinician do not trigger attribution for that measure. The 2026 TPCC modification adds a specific exclusion: ACP TIN-NPI candidate events are excluded when all non-ACP TIN-NPIs in the group are specialty-excluded from TPCC.
How Does TPCC Attribution Differ from Episode-Based Attribution?
TPCC attribution and episode-based attribution use different triggers, time windows, and attribution logic. The table below compares the two approaches across key attribution dimensions.
| Dimension | TPCC Attribution | Episode-Based Attribution |
|---|---|---|
| Attribution trigger | Plurality of primary-care E/M visits across the performance year | A single procedure or condition trigger code |
| Time window | Full performance year (12 months) | Condition- or procedure-specific episode window |
| Attribution unit | TIN-NPI with the most primary-care E/M visits for the patient | TIN-NPI that billed the trigger code |
| Typical clinician attributed | Primary care physician or ACP with the highest E/M visit share | Surgeon, hospitalist, or specialist who performed the trigger procedure |
Worked attribution example: A Medicare patient undergoes total hip replacement surgery. The surgeon’s TIN-NPI billed the hip arthroplasty CPT code, so the surgeon is attributed the Hip Replacement episode-based measure cost for that patient. The same patient sees a primary-care physician for annual management throughout the year.
The primary-care physician’s TIN-NPI holds the plurality of primary-care E/M visits, so the primary-care physician is attributed TPCC cost for that same patient. One patient generates two separate cost attributions to two different TIN-NPIs.
What Is the TIN-NPI Level in MIPS Cost Attribution?
The TIN-NPI is the attribution unit CMS uses for MIPS Cost. A TIN-NPI is the pairing of a clinician’s individual National Provider Identifier (NPI) with the Tax Identification Number (TIN) of the practice or group through which the clinician billed Medicare. Cost attribution sits at the TIN-NPI level: if the same NPI bills under two different TINs during the performance year, each TIN-NPI pair accumulates attribution and scoring separately.
TIN-NPI-level attribution matters most for clinicians who practice at multiple locations or switch groups mid-year. Each TIN-NPI combination produces a separate Cost performance result. Group-level reporting combines the TIN-NPI results of all clinicians billing under the group TIN into a single group-level Cost score.
Can Clinicians Dispute MIPS Cost Attribution?
Yes. Clinicians can dispute MIPS Cost attribution through the CMS Targeted Review process after the MIPS Final Score is released. Common grounds for a Targeted Review request include incorrect TIN-NPI attribution (for example, claims billed under the wrong TIN), specialty exclusion rules misapplied to the clinician, and candidate events miscoded in the underlying Medicare claims data. Targeted Review requests are submitted through the QPP Help Desk after final scores are published each year.
How Is Risk Adjustment Applied to MIPS Cost?
Risk adjustment normalizes raw cost figures for patient mix so that clinicians treating sicker or more complex patients are not penalized for the higher costs associated with that population. CMS applies risk adjustment to MIPS Cost scores using Hierarchical Condition Category (HCC) scores, demographic factors, and dual-eligibility status.
Risk adjustment operates at the measure level: each attributed patient’s expected cost is adjusted before comparing actual cost to the performance-period benchmark.
Without risk adjustment, a primary-care practice serving a high-acuity geriatric population would consistently show higher raw costs than a practice serving healthier Medicare patients, even with identical care quality. Risk adjustment corrects for that population-mix difference before scoring.
What Is a Hierarchical Condition Category (HCC) Score?
A Hierarchical Condition Category (HCC) score is a CMS-administered risk model that converts a patient’s ICD-10 diagnosis codes into a numeric risk score. Higher HCC scores indicate greater patient complexity and higher expected Medicare costs. CMS uses HCC scores as the primary input for MIPS Cost risk adjustment: each attributed patient’s HCC score raises or lowers the expected cost against which the clinician’s actual cost is measured.
HCC scores are built from diagnosis codes submitted on Medicare claims during the measurement period. Incomplete ICD-10 documentation leads to lower HCC scores and underestimated expected costs.
What Demographic Factors Affect MIPS Cost Risk Adjustment?
Four demographic factors apply to MIPS Cost risk adjustment alongside HCC scores. Each factor adjusts the expected cost for a given patient up or down before comparison to the benchmark:
- Age: Older Medicare beneficiaries carry higher expected costs, and risk adjustment incorporates age-related cost increases across the attributed patient population.
- Sex: Sex-specific cost differences are incorporated into the CMS risk adjustment model and applied at the individual patient level.
- Dual-eligibility (Medicare + Medicaid): Beneficiaries enrolled in both Medicare and Medicaid (dual-eligible beneficiaries) carry higher expected costs due to greater social and clinical complexity.
- Medicaid-status interactions with HCC: Dual-eligibility status interacts with HCC scores to produce a combined adjustment that reflects the compounding effect of clinical and social complexity on expected cost.
Dual-eligible beneficiaries add the most meaningful adjustment complexity and are the most significant demographic factor for practices serving low-income or underserved populations.
Does Risk Adjustment Guarantee a Fair MIPS Cost Score?
No, risk adjustment normalizes Cost scores for HCC-coded complexity, age, sex, and dual eligibility, but risk adjustment does not capture every clinical or social risk factor that drives Medicare cost. Social determinants of health, undocumented chronic conditions, and geographic care-access differences are not fully reflected in HCC-based models.
Practices serving complex populations should validate HCC coding completeness annually to confirm that risk adjustment operates on an accurate diagnosis record.
How Is the MIPS Cost Category Score Calculated?
The Cost category percent score is the average of all measure-level scores attributed to the clinician, expressed as a percentage. Each measure-level score runs on a scale of 1 to 10, reflecting how the clinician’s actual cost compares to the performance-period benchmark for that measure.
The Cost category percent score is then multiplied by the 30% weight to produce the Cost category’s point contribution to the MIPS Final Score. Cost benchmarks use performance-period data, not historical data. The table below shows a simplified three-measure scoring example.
| Measure | Attributed Cases | Measure Score (1-10) | Weighted Contribution |
|---|---|---|---|
| TPCC | 45 patients | 7.2 | Part of the average cost percent score |
| Hip Replacement (episode-based) | 28 episodes | 8.1 | Part of the average cost percent score |
| MSPB Clinician | 6 episodes | 4.5 | Part of the average cost percent score |
| Cost Category Percent Score | (7.2 + 8.1 + 4.5) / 3 = 6.6 / 10 x 100 = 66% | 66% x 30% = 19.8 MIPS points |
CMS publishes Cost performance feedback through the QPP portal after the performance year closes. Clinicians can review measure-level scores, attributed case counts, and benchmark comparisons in the annual Cost feedback report.
What Is the 20-Case Minimum for MIPS Cost Scoring?
A cost measure requires at least 20 attributed cases before CMS scores the measure against the benchmark. For TPCC, a case is an attributed patient. For episode-based measures, a case is an attributed episode. If the attributed count falls below 20 for a given measure, CMS excludes that measure from the Cost category score calculation entirely.
Low-volume specialties or practices in smaller markets may fall below the 20-case minimum on certain episode-based measures. In that situation, the measure is dropped from the clinician’s Cost category score without penalty. Only measures with 20 or more attributed cases enter the average that produces the Cost category percent score.
Did the MIPS Cost Category Weight Change for 2026?
No, CMS held the Cost category weight at 30 percent of the MIPS Final Score, unchanged from 2025, per the November 5, 2025, Physician Fee Schedule Final Rule. The four-category weight distribution for 2026 is: Cost 30%, Quality 30%, Promoting Interoperability 25%, and Improvement Activities 15%. The Cost weight has remained at 30% since the category reached full weighting under MACRA.
What Changed for MIPS Cost in 2026?
CMS finalized four Cost-category updates for 2026 in the November 5, 2025, Physician Fee Schedule Final Rule. The updates cover the TPCC measure design, the scoring-eligible measure count, the treatment of newly-finalized measures, and benchmark methodology:
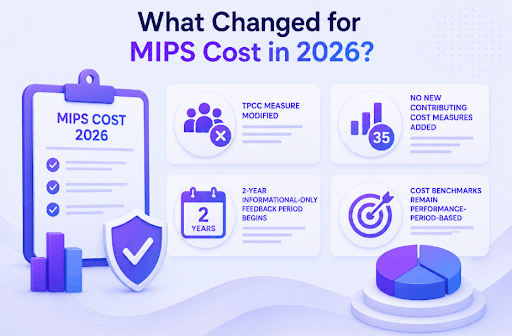
- TPCC measure modified: Candidate events initiated by ACP TIN-NPIs are excluded when all non-ACP TIN-NPIs in the group are specialty-excluded from TPCC.
- No new contributing cost measures added: The 35 scoring-eligible measures are unchanged from 2025. One new claims-based measure was finalized but carries informational-only status.
- 2-year informational-only feedback period begins: Any new cost measure finalized beginning with PY 2026 enters a 2-year informational period before scoring.
- Cost benchmarks remain performance-period-based: CMS did not shift Cost benchmarks to a historical-data basis for 2026.
Which 2026 Cost Change Matters Most for Clinicians?
The TPCC modification matters most for groups with mixed physician-ACP staffing. If a group practice includes physicians who are specialty-excluded alongside ACPs who previously triggered TPCC attribution, the 2026 rule change may reduce or eliminate TPCC attribution for that group. Groups in this situation should audit their TIN-NPI composition and run an attribution review before the performance year ends to understand the practical exposure.
The 2-year informational-only feedback period carries zero immediate scoring impact because the only new measure finalized for 2026 already enters informational-only status automatically. The remaining two changes (no new contributing measures; benchmark methodology unchanged) are procedural confirmations with minimal operational effect on 2026 Cost scores.
How Does the 2-Year Informational-Only Feedback Period Work?
Beginning with performance year 2026, any new cost measure CMS finalizes enters a 2-year informational-only feedback period before contributing to the Cost category score. The three-stage timeline for a new measure runs as follows:
| Year | Status | Score Impact |
|---|---|---|
| Year of finalization (PY 2026 or later) | Informational-only | No contribution to Cost score or MIPS Final Score |
| Year 2 | Informational-only | No contribution to Cost score or MIPS Final Score |
| Year 3 onward | Standard scoring | Contributes to the Cost category percent score |
Clinicians receive performance feedback on new-measure results during the two informational years. That feedback allows practices to understand cost position and adjust care coordination patterns before the measure carries scoring weight. The 2-year buffer applies only to measures newly finalized after 2026; existing measures (TPCC, MSPB Clinician, and the 32 episode-based measures) continue under standard scoring in 2026.
How Can a Practice Influence MIPS Cost Performance?
Even though CMS calculates MIPS Cost, clinicians influence performance through five indirect levers. Each lever targets a specific cost mechanism within the attribution model:
- Complete HCC Coding: Accurate ICD-10 documentation confirms that HCC scores reflect true patient complexity. Incomplete HCC coding produces lower risk adjustment and makes actual costs appear higher relative to expected costs, lowering the Cost measure score.
- Coordinate Post-acute Placement: Placement decisions after hospitalization (skilled nursing facility, home health, or self-managed recovery) directly affect episode costs for episode-based measures and MSPB Clinician, because post-discharge claims fall inside the episode window.
- Manage Referral Patterns: Referrals to in-network or value-based specialists reduce fragmentation costs that fall inside the attribution windows of TPCC and episode-based measures.
- Follow Up After Hospital Discharge: Timely post-discharge primary-care visits reduce readmission risk and the associated claims that accumulate inside MSPB Clinician and episode-based episode windows.
- Document Primary-care Visits Fully: Complete primary-care visit documentation supports both HCC accuracy and TPCC attribution. Underdocumented visits may not qualify as primary-care E/M visits, reducing the visit count that determines TPCC attribution.
How Does Macralytics Monitor MIPS Cost Attribution and Risk?
Macralytics reviews MIPS Cost attribution accuracy using QPP feedback reports, validates HCC coding completeness against the attributed patient population, and identifies episode-based measure exposures before the performance year closes. The review process checks TIN-NPI-level attribution results, flags candidate events that may be subject to specialty exclusion, and confirms that risk adjustment inputs align with the practice’s actual patient complexity.
Practices that complete an attribution review before year-end have time to correct documentation gaps and request a Targeted Review if attribution errors are identified after final-score release. For details on how we monitor MIPS Cost performance, visit the Macralytics QPP services page.
Do MIPS Value Pathway (MVP) Cost Measures Match Traditional MIPS Cost Measures?
Partial. MIPS Value Pathways (MVPs) draw from the same 35-measure inventory used in traditional MIPS, but MVP participants receive a specialty-aligned subset of those measures rather than the full set. The attribution rules for MVP Cost differ from traditional MIPS Cost attribution because MVPs apply MVP-specific candidate-event logic aligned to each pathway’s specialty focus.
The underlying measure logic for TPCC, MSPB Clinician, and the 32 episode-based measures is unchanged across both pathways. The subset of measures scored and the attribution path that leads to each score differ between traditional MIPS and MVP reporting.
The MIPS Cost category is the CMS-calculated, claims-based 30%-weighted component of the MIPS Final Score that measures resource use across 35 measures for the 2026 performance year. Clinicians submit no Cost data; attribution and scoring run automatically from Medicare Part B claims.

Schedule your free MIPS consultation.
Drop your work email and a certified MIPS consultant will reach out to schedule a personalized consultation, no obligation.