MIPS Quality Measures: Selection, Scoring, and Bonuses
MIPS Quality measures are the clinical-care performance measures CMS uses to score the Quality category, the largest component of the MIPS final score at 30 percent in 2026. Under the Merit-Based Incentive Payment System (MIPS), clinicians select six measures(including at least one outcome or high-priority measure) from approximately 187finalized for the 2026 performance year.
Each measure requires data on 75 percent of eligible encounters, submitted through a Registry, QCDR, eCQM, or Medicare Part B claims. Each measure earns 1 to 10 points on decile benchmarks.
What Are MIPS Quality Measures?
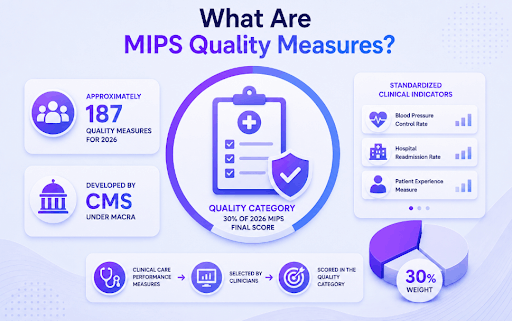
MIPS Quality measures are the clinical-care performance measures the Centers for Medicare and Medicaid Services (CMS) uses to score the Quality category of MIPS, one of four MIPS performance categories under the Quality Payment Program (QPP). The Quality category is weighted at 30 percent ofthe 2026 MIPS final score. CMS finalized approximately 187 quality measures forthe 2026 performance year under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA).
Each quality measure is a standardized clinical indicator, such as blood-pressure control rate or hospital readmission rate, assigned a measure ID by CMS. Clinicians select measures from the full inventory based on specialty, patient population, and reporting mechanism. The Quality category percent score feeds up to 30 points into the 100-point MIPS Final Score.
How Do Quality Measures Contribute to the MIPS Final Score?
The Quality category contributes up to 30 points to the 100-point MIPS Final Score. CMS calculates a Quality category percent score using earned achievement points across all submitted measures. That percent score is multiplied by the 30% weight to produce the Quality category’s contribution to the MIPS Final Score. The four-category weight distribution for 2026 is: Quality 30%, Cost 30%, Promoting Interoperability 25%, and Improvement Activities 15%.
The MIPS performance threshold for 2026 is 75 points. Clinicians scoring at or above 75 points earn a positive Medicare Part B payment adjustment. Clinicians below that threshold face a negative adjustment of up to 9 percent. The three Quality bonus paths (small-practice, complex-patient, and improvement scoring) all help clinicians clear or exceed the 75-point threshold.
How Many Quality Measures Does CMS Publish for 2026?
CMS finalized approximately 187 quality measures for the 2026 performance year per the November 5, 2025, Physician Fee Schedule Final Rule. The 2026 inventory reflects 5 newly added measures, 10 measures retired from 2025, and 30 measures that received substantive modifications. Additional measures approved outside rulemaking by Qualified Clinical Data Registry (QCDR) vendors supplement the 187-measure base inventory.
The 187-measure count represents the pool from which clinicians select their 6 reporting measures. Not every measure applies to every specialty or care setting. Specialty measure sets group pre-selected measures relevant to a given specialty, narrowing the selection decision for clinicians whose patient mix matches an available set.
Did MIPS Quality Measures Change for 2026?
Yes, CMS finalized 5 new measures, retired 10, substantively modified 30, and removed “health equity” from the high-priority measure definition for the 2026 performance year. The total inventory remained near 187 after accounting for additions and retirements. The full breakdown of 2026 Quality changes, including which measures were retired and which were modified, is detailed in the H2.6 section below.
How Do Clinicians Select MIPS Quality Measures?
Clinicians select MIPS Quality measures through two paths: individual measure selection (choosing 6 from the full ~187 inventory, including at least 1 outcome or high-priority measure) or submission of a complete specialty measure set in lieu of individual selection. The Eligible Measure Applicability (EMA) process applies when a clinician’s specialty or case mix does not support 6 applicable measures.
Measure selection determines the scoring ceiling for the Quality category. Choosing measures where the clinician’s performance rates exceed national benchmarks produces more achievement points per measure. Topped-out measures cap at 7 points regardless of performance rate, so measure selection directly affects the maximum attainable Quality category percent score.
What Is the 6-Measure Selection Rule?
Clinicians reporting under traditional MIPS select 6 measures from the full Quality measure inventory for the 2026 performance year. At least 1 of the 6 measures must be an outcome measure. If no applicable outcome measure exists for the clinician’s case mix, at least 1 measure must be a high-priority measure instead. All 6 selected measures are reported across the full calendar-year performance period (January 1 through December 31, 2026).
Selecting 6 measures that the clinician can consistently exceed on decile benchmarks produces the highest Quality category percent score. Measures with flat benchmarks (topped-out measures) cap at 7 points and reduce the maximum possible achievement. Measure selection is the single highest-impact decision point in MIPS Quality preparation.
What Counts as an Outcome or High-Priority Measure?
Outcome measures track the direct clinical results of patient care, such as HbA1c control rate (Measure #1), blood-pressure control in patients with hypertension (Measure #236), or 30-day hospital readmission rate. High-priority measures cover patient experience, appropriate use, patient safety, resource use, and care coordination. For the 2026 performance year, CMS removed “health equity” from the high-priority measure definition per the November 5, 2025, Physician Fee Schedule Final Rule.
The distinction matters for selection compliance. Submitting 6 measures without at least 1 outcome (or 1 high-priority if no outcome applies) results in a selection penalty under CMS scoring rules. CMS publishes a measure-type flag in the QPP Quality measure specifications to identify which measures qualify as outcome or high-priority.
How Does a Specialty Measure Set Differ from Individual Measure Selection?
A specialty measure set is a pre-built list of Quality measures that CMS or a QCDR vendor assembles for a defined specialty, such as Cardiology, Orthopedic Surgery, or Internal Medicine. Clinicians who submit the complete specialty measure set report every measure in that set rather than choosing 6 individually. Specialty sets reduce the effort of selection by removing the need to evaluate 187 measures.
The table below compares the two selection paths across key dimensions:
| Dimension | Individual Selection | Specialty Measure Set |
|---|---|---|
| Measure count | 6 measures chosen from ~187 inventory | All measures in the pre-built specialty set |
| Outcome requirement | At least 1 outcome or high-priority measure | Set satisfies outcome requirement if built to spec |
| Flexibility | High — clinician selects measures targeting higher decile performance | Low — measure list is fixed by the set |
| Best fit | Clinicians with varied case mix or multiple specialties | Clinicians whose patient mix maps cleanly to one specialty |
If a specialty measure set contains fewer than 6 measures, the clinician submits all measures in the set. CMS scores the clinician on the full set without penalizing the smaller measure count.
What Is the 75% Data Completeness Requirement?
Each selected MIPS Quality measure requires performance or exception data on at least 75 percent of denominator-eligible encounters across the 2026 performance year. A measure that falls below 75% data completeness scores zero points, regardless of the clinician’s actual performance rate on the encounters that were reported. The 75% data completeness threshold is unchanged from 2025 per the November 5, 2025 Final Rule.
Data completeness affects every reporting mechanism. Registry and QCDR vendors track completeness in real time during the performance year, allowing clinicians to identify measures at risk before the submission window opens. Claims-based reporters must rely on practice billing data to estimate completeness before the final submission deadline.
Can a Clinician Report Fewer Than Six MIPS Quality Measures?
Yes, in limited cases. The Eligible Measure Applicability (EMA) process allows CMS to score a clinician fairly when fewer than 6 applicable measures exist for the clinician’s specialty or case mix. EMA applies automatically when the QPP system identifies that a clinician’s patient population does not support 6 eligible measures. Outside EMA-qualifying situations, reporting 6 measures (including at least 1 outcome or high-priority measure) is the standard rule for traditional MIPS reporting.
How Are MIPS Quality Measures Scored?
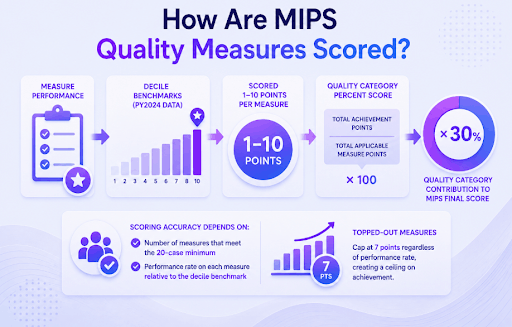
MIPS Quality measures are scored 1 to 10 points per measure on decile benchmarks derived from PY2024 actual performance data. The Quality category percent score equals total achievement points divided by total applicable measure points, multiplied by 100. That percent score is then multiplied by the 30% weightto produce the Quality category’s contribution to the MIPS Final Score.
Scoring accuracy depends on two variables: the number of measures that meet the 20-case minimum, and the performance rate on each measure relative to the decile benchmark. Topped-out measures cap at 7 points regardless of performance rate, creating a ceiling on achievement from those measures.
What Is a Decile Benchmark?
A decile benchmark divides the national performance distribution for a given Quality measure into 10 equal buckets using actual submitted data from the PY2024 performance year. A clinician’s performance rate on the measure is compared to those 10 deciles to assign a point score from 1 (lowest decile) to 10 (highest decile). Performing at the top decile on a measure earns the maximum 10 points for that measure.
Decile benchmarks are calculated separately for each measure and for each reporting mechanism (Registry, QCDR, eCQM, claims). A clinician switching from claims-based to Registry reporting may land in a different decile for the same performance rate because the benchmark populations differ by mechanism. The 2026 benchmarks use PY2024 submitted data, published annually by CMS through the QPP resource library.
How Is the Quality Category Percent Score Calculated?
The Quality category percent score is calculated using this formula: Quality % Score = (Total Achievement Points / Total Applicable Measure Points) x 100. That result is then multiplied by the 30% weight to produce the category’s contribution to the MIPS Final Score. Quality Improvement Scoring, if applicable, adds up to 10 percentage points to the Quality % Score before the weight multiplication.
Worked example: A clinician submits 6 measures, all meeting the 20-case minimum. Decile scores earned per measure: 8, 7, 6, 9, 5, 8. Total achievement points = 43. Total applicable measure points = 60 (6 measures x 10 points each). Quality % Score = 43 / 60 x 100 = 71.7%. Weighted Quality contribution = 71.7% x 30% = 21.5 of 30 available Quality points toward the MIPS Final Score.
What Is the 20 Denominator-Eligible Case Minimum?
A MIPS Quality measure requires at least 20 denominator-eligible cases before CMS scores the measure against the national benchmark. A denominator-eligible case is a patient encounter that qualifies under the measure’s denominator criteria. If the attributed case count falls below 20 for a given measure, CMS excludes the measure from the Quality category score entirely without applying a scoring penalty for the exclusion.
Low-volume specialties or practices in smaller markets commonly fall below the 20-case threshold on some selected measures. In that situation, only the measures with 20 or more eligible cases contribute to the Quality % Score. Selecting measures with sufficient patient volume in the practice’s case mix reduces the risk of exclusion.
What Happens When a MIPS Quality Measure Becomes Topped-Out?
A topped-out measure is one where the national performance distribution shows that most clinicians already perform at or near the top of the benchmark range. CMS applies a 7-point cap to topped-out measures: regardless of performance rate, no clinician earns more than 7 points on a topped-out measure in 2026.
Certain topped-out measures use a flat-benchmarking methodology, which replaces the decile structure with a fixed performance-rate-to-points table. Clinicians holding topped-out measures in their 6-measure selection face a lower maximum Quality % Score than clinicians holding non-topped-out measures. Reviewing the topped-out designation annually, which CMS updates with each Final Rule, is part of effective measure selection strategy.
Are All MIPS Quality Measures Weighted Equally?
Yes. Within the Quality category, each selected measure earns up to 10 points on its decile benchmark regardless of measure ID, specialty category, or clinical complexity. A measure’s contribution to the Quality category percent score equals its earned points divided by the total applicable measure points across all submitted measures. The single exception applies to topped-out measures, which cap at 7 points instead of 10.
What MIPS Quality Bonuses Can Clinicians Earn?
Three bonus paths exist under MIPS Quality for the 2026 performance year. The small-practice bonus adds +6 points directly to the MIPS Final Score. The complex-patient bonus adds up to +10 points to the MIPS Final Score. The Quality Improvement Scoring bonus adds up to +10 percentage points to the Quality category percent score before the 30% weight is applied. All three bonuses are stacked in the table below.
| Bonus | Maximum Value | Applied To | Eligibility Gate |
|---|---|---|---|
| Small-practice bonus | +6 points | MIPS Final Score | TIN with 15 or fewer clinicians; at least 1 Quality measure submitted |
| Complex-patient bonus | Up to +10 points | MIPS Final Score | HCC risk score and dual-eligible ratio at or above the median threshold |
| Quality Improvement Scoring | Up to +10 percentage points | Quality category percent score | Year-over-year improvement in Quality achievement from prior performance year |
All three bonuses are calculated automatically by CMS from submitted data. No separate bonus application is required. Stacking all three is possible when a small practice serving a complex patient population also shows year-over-year Quality improvement.
What Is the Small-Practice Bonus?
The small-practice bonus adds +6 points directly to the MIPS Final Score for practices with a Tax Identification Number (TIN) covering 15 or fewer eligible clinicians. The bonus is triggered automatically when the small practice submits at least one Quality measure for the performance year. No separate application, attestation, or threshold of Quality performance is required to receive the small-practice bonus.
The small-practice bonus applies at the TIN level. A solo clinician billing under a TIN alone qualifies. A group practice with 16 or more clinicians billing under the same TIN does not qualify. The +6 points are added to the MIPS Final Score after all four category scores are combined and weighted.
How Does the Complex-Patient Bonus Work?
The complex-patient bonus adds up to +10 points to the MIPS Final Score based on the complexity of the clinician’s attributed patient population. CMS calculates the bonus using two inputs: the average Hierarchical Condition Category (HCC) risk score across attributed patients, and the proportion of dual-eligible beneficiaries (patients enrolled in both Medicare and Medicaid) in the attributed population. Clinicians at or above the national median on both inputs receive the full bonus.
The complex-patient bonus addresses the structural disadvantage that clinicians serving high-acuity or socially vulnerable populations face in cost and quality performance scoring. The bonus applies at the TIN-NPI level. It does not require any action from the clinician and is calculated automatically from Medicare claims and enrollment data after the performance year ends.
What Is the Quality Improvement Scoring Bonus?
Quality Improvement Scoring adds up to +10 percentage points to the Quality category percent score when the clinician’s year-over-year Quality achievement improves. The improvement bonus formula is: Improvement Points = 10 x (Current Year Achievement Points – Prior Year Achievement Points) / Prior Year Achievement Points. The result is capped at 10 percentage points and added to the Quality % Score before the 30% weight is applied.
Unlike the small-practice and complex-patient bonuses, the Quality Improvement Scoring bonus is added to the Quality category percent score, not to the MIPS Final Score directly. The impact on the MIPS Final Score equals the improvement percentage points multiplied by the 30% weight. A clinician earning the full 10-percentage-point improvement bonus gains an additional 3 points on the MIPS Final Score.
Is the Small-Practice Bonus Applied to MIPS Quality Alone?
No, the +6 small-practice bonus is added to the MIPS Final Score, not to the Quality category percent score. The bonus applies to the total MIPS Final Score regardless of individual category performance, as long as the small practice submits at least one Quality measure. The bonus applies regardless of the practice’s Cost, Promoting Interoperability, or Improvement Activities scores.
How Do Clinicians Report MIPS Quality Data?
Clinicians report MIPS Quality data through five CMS-approved mechanisms for the 2026 performance year. The selected reporting mechanism determines the available measure inventory, the benchmark population used for scoring, and the data completeness tracking method.
Reporting mechanism selection affects score outcomes independently of measure selection. The same measure may benchmark differently across mechanisms because CMS calculates separate decile benchmarks for each mechanism using that mechanism’s submitted data from PY2024.
What Are the Five MIPS Quality Reporting Mechanisms?
CMS approves five reporting mechanisms for MIPS Quality data submission in 2026. Each mechanism supports a different collection type and fits a different practice profile:
| Mechanism | Collection Type | Best Fit | 2026 Status |
|---|---|---|---|
| Qualified Registry | MIPS CQM | Groups of any size, widest measure access | Active |
| Qualified Clinical Data Registry (QCDR) | MIPS CQM (specialty-aligned) | Specialty practices with QCDR-specific measures | Active |
| EHR (eCQM) | eCQM via CEHRT | Practices with Certified Electronic Health Record Technology (CEHRT) | Active |
| Medicare Part B Claims | Claims-based measure | Small practices only (15 or fewer clinicians) | Active (small practice only) |
| CMS Web Interface | Group-level web submission | Large groups; limited measure set | Deprecated for most; limited eligibility |
Qualified Registry reporting offers the broadest measure access across all practice sizes. Claims-based reporting is restricted to small practices (15 or fewer clinicians) and covers a limited subset of MIPS Quality measures available through the claims mechanism.
How Does eCQM Differ from MIPS CQM?
An electronic Clinical Quality Measure (eCQM) is collected directly from Certified Electronic Health Record Technology (CEHRT)-certified EHR data using standardized eCQM logic specifications published by CMS. A MIPS CQM (Clinical Quality Measure) is collected through a Qualified Registry or QCDR using measure-specific data submission that does not require CEHRT certification.
Both measure types can cover the same underlying clinical concept, but the collection mechanism, data source, and benchmark population differ. Clinicians using CEHRT-equipped EHR systems can choose eCQM reporting, which eliminates the need for a separate Registry vendor. Practices without CEHRT or with EHR systems that do not support eCQM export use MIPS CQM reporting through a Registry or QCDR.
Decile benchmarks for eCQMs and MIPS CQMs are calculated separately, so a clinician’s point score for the same clinical measure may differ across collection types.
When Does Registry Reporting Outperform Claims-Based Reporting?
Registry reporting produces higher Quality scores than claims-based reporting in four specific scenarios:
- The practice has 16 or more clinicians, claims-based reporting is restricted to small practices only, so Registry is the only available mechanism for larger groups.
- Higher-decile measures are accessible only via Registry, the claims measure inventory is a subset of the full Registry measure list.
- The Registry vendor offers real-time benchmark gap reporting Registry vendors alert clinicians to low-performing measures during the year, allowing corrective action before submission.
- The practice submits a hybrid eCQM/Registry report, some clinicians combine eCQM and Registry submissions across their 6 measures to access the broadest benchmark set.
Claims-based reporting carries the advantage of zero Registry vendor cost and no additional data collection infrastructure. For practices that qualify and whose claims already reflect the required quality indicators, claims reporting is the lowest-overhead option.
What Changed for MIPS Quality in 2026?
CMS finalized 2026 Quality category updates in the November 5, 2025 Physician Fee Schedule Final Rule. Four changes affect measure selection, scoring, and reporting for the 2026 performance year:
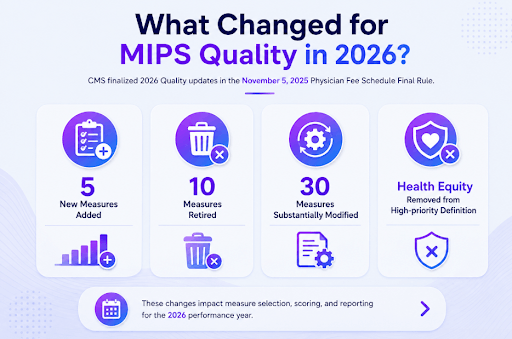
- 5 New Measures Added: CMS added 5 measures to the 2026 Quality inventory. The full list appears in the Final Rule and the QPP Quality measure specifications published annually by CMS.
- 10 Measures Retired: Ten measures were removed from the 2026 inventory. Clinicians who reported any of the 10 retired measures in 2025 must replace those measures with eligible 2026 alternatives.
- 30 Measures Substantively Modified: CMS revised measure specifications, denominator definitions, or performance benchmarks for 30 existing measures. Practices that track measure performance internally must review updated 2026 specifications before the performance year begins.
- Health Equity Removed from High-priority Definition: CMS removed “health equity” as a qualifying category for high-priority measure designation for 2026. Clinicians relying on a health equity measure to satisfy the 1 outcome/high-priority requirement must confirm the measure retains high-priority status or identify a replacement.
Which MIPS Quality Measures Were Retired for 2026?
Ten MIPS Quality measures were retired for the 2026 performance year per the November 5, 2025 Physician Fee Schedule Final Rule. Examples of retired measures include:
- Measure #185 (Colonoscopy Interval for Patients with a History of Adenomatous Polyps)
- Measure #264 (Sentinel Lymph Node Biopsy for Invasive Breast Cancer)
- Measure #322 (Cardiac Stress Imaging Not Meeting Appropriate Use Criteria for Low-Risk Surgery)
- Measure #443 (Non-Recommended Cervical Cancer Screening in Adolescent Females)
- Measure #487 (Screening for Social Drivers of Health), and Measure #508 (Adult COVID-19 Vaccination Status).
Clinicians who selected any retired measure in their 2025 set must rebuild their 6-measure selection for 2026. The full retired-measure list lives on the 2026 MIPS Quality measures page at /quality/measures/ and in the QPP Quality measure specifications document published by CMS after Final Rule release each year.
Did MIPS Quality Data Completeness Change for 2026?
No. CMS held the data completeness threshold at 75 percent of denominator-eligible encounters for the 2026 performance year, unchanged from 2025 per the November 5, 2025 Physician Fee Schedule Final Rule. Measures that fall below 75% data completeness score zero points regardless of the actual performance rate on reported encounters.
How Does Macralytics Support MIPS Quality Measure Selection and Submission?
Macralytics runs measure-selection audits by modeling each practice’s patient mix against the full 2026 Quality measure inventory. The audit identifies which measures the practice’s case data supports, projects the decile score range for each eligible measure using PY2024 benchmarks, and flags any topped-out measures that cap at 7 points. Macralytics then manages data-completeness monitoring through the performance year and submits final Quality data through the Macralytics Qualified Registry.
The selection audit process identifies the 6-measure combination with the highest projected Quality category percent score before the performance year begins, not after submission closes. Practices that complete a measure-selection audit in Q4 of the prior year or Q1 of the performance year have the full year to collect qualifying encounters on the optimal measure set.
Do MIPS Quality Measures Apply to MIPS Value Pathway (MVP) Reporting?
Yes. MIPS Value Pathways (MVPs) include Quality measures as a required component, but MVP reporting uses 4 Quality measures instead of the 6 required under traditional MIPS. The 4 MVP Quality measures are drawn from the MVP’s pre-defined specialty-aligned subset rather than the full ~187-measure inventory.
At least 1 of the 4 measures must be an outcome measure. The decile-benchmark scoring method (1 to 10 points per measure) applies unchanged across both traditional MIPS and MVP reporting. MVP-specific Quality measures share the same underlying clinical concepts as traditional MIPS measures but are pre-selected by CMS to match the clinical focus of each MVP. Clinicians who participate in an MVP cannot substitute measures from outside the MVP’s pre-defined subset.
The Quality category weight (30% of the MIPS Final Score) and the data completeness requirement (75% of eligible encounters) apply equally to MVP and traditional MIPS Quality reporting. MIPS Quality measures are the clinical-care performance measures CMS uses to score the Quality category, the 30%-weighted component of the MIPS Final Score for approximately 187 finalized measures in 2026.

Schedule your free MIPS consultation.
Drop your work email and a certified MIPS consultant will reach out to schedule a personalized consultation, no obligation.